

Pierre Quartier
immunologie, hématologie et rhumatologie pédiatriques,
hôpital Necker ; Enfants-Malades,
149, rue de Sèvres,
75015 Paris,
France Adresse e-mail : quartier@necker.fr (P. Quartier)
Reçu le 21 mars 2006
Accepté le 5 juillet 2006
Disponible sur internet le 10 novembre 2006
Éditorial / Revue du Rhumatisme 74 (2007)
When should we use TNF antagonists in children with rheumatic disease?
1. Introduction
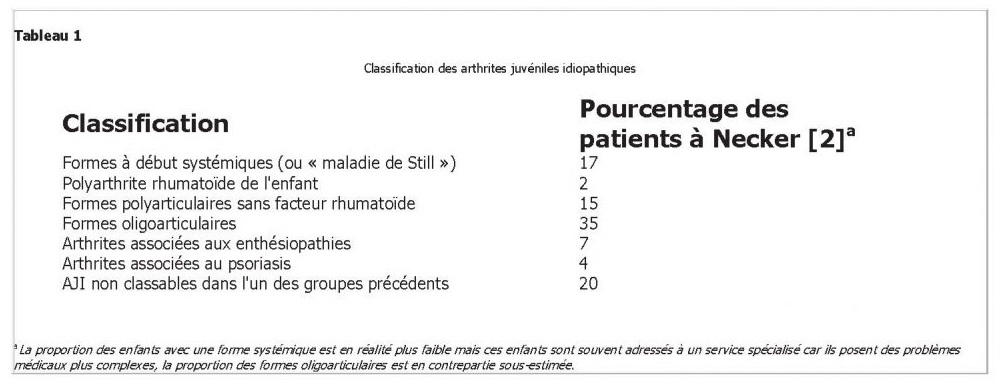
 Les arthrites juvéniles idiopathiques (AJI), antérieurement appelées arthrites chroniques juvéniles (ACJ), représentent un ensemble hétérogène d’affections dont les caractéristiques communes sont un début de la maladie avant l’âge de 16 ans et l’existence d’une arthrite d’une durée d’au moins six semaines sans cause reconnue (on doit exclure une infection, une maladie maligne, une arthrite réactionnelle, …) [1]. Comme indiqué dans le Tableau 1, il y a en fait plusieurs formes d’AJI très différentes et seuls 2 % des enfants ont une polyarthrite rhumatoïde (PR), comme les adultes (et il s’agit surtout d’adolescentes) [2].
Les arthrites juvéniles idiopathiques (AJI), antérieurement appelées arthrites chroniques juvéniles (ACJ), représentent un ensemble hétérogène d’affections dont les caractéristiques communes sont un début de la maladie avant l’âge de 16 ans et l’existence d’une arthrite d’une durée d’au moins six semaines sans cause reconnue (on doit exclure une infection, une maladie maligne, une arthrite réactionnelle, …) [1]. Comme indiqué dans le Tableau 1, il y a en fait plusieurs formes d’AJI très différentes et seuls 2 % des enfants ont une polyarthrite rhumatoïde (PR), comme les adultes (et il s’agit surtout d’adolescentes) [2].
Les anti-inflammatoires non stéroïdiens restent le traitement de première ligne. Ils sont utilisés seuls ou en association aux infiltrations articulaires de corticostéroïdes et à la kinésithérapie dans les formes peu sévères. Le méthotrexate est comme dans la PR de l’adulte le traitement de seconde ligne de choix des formes polyarticulaires ou des formes oligoarticulaires qui ont secondairement une évolution polyarticulaire mais environ 30 % des patients ne tolèrent pas ce traitement ou ont une réponse insatisfaisante. Les corticostéroïdes sont le plus souvent très efficaces sur les symptômes mais leur prescription sur le long cours en pédiatrie est à l’origine de complications multiples incluant le retard de croissance. Leur utilisation prolongée n’est donc à considérer qu’en l’absence de toute alternative thérapeutique. Les biothérapies et tout particulièrement les anti-TNFα sont utilisés chez l’enfant depuis la fin des années 1990 et ont transformé l’évolution des formes sévères d’AJI [3–6]. Certaines formes d’AJI et notamment les formes systémiques sont cependant moins sensibles aux anti-TNFα et semblent mieux répondre à des anticytokines ciblant des molécules qui semblent plus particulièrement incriminées dans cette maladie et d’autres syndromes auto-inflammatoires comme l’interleukine (IL)-1 ou l’IL-6 [7,8].
2. Principaux anti-TNF et expérience acquise en pédiatrie
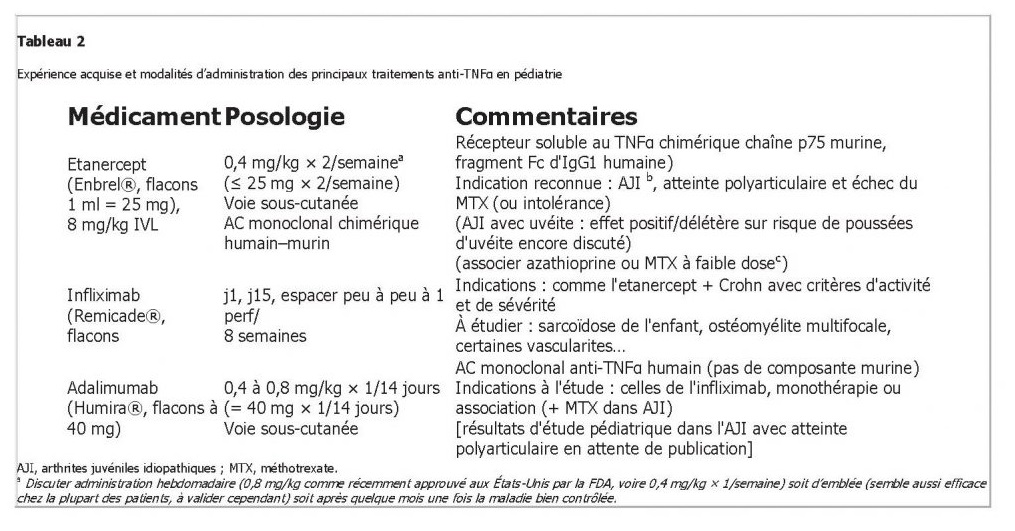
Trois anti-TNFα ont été utilisés dans les AJI et dans quelques autres indications chez l’enfant (Tableau 2). Dans l’AJI, l’efficacité et la tolérance de l’etanercept et de l’infliximab semblent similaires, cependant seul le premier a actuellement une autorisation de mise sur le marché (AMM). Peu de données sont disponibles pour l’adalimumab, introduit plus récemment.
3. Prescrire un anti-TNF en rhumatologie pédiatrique
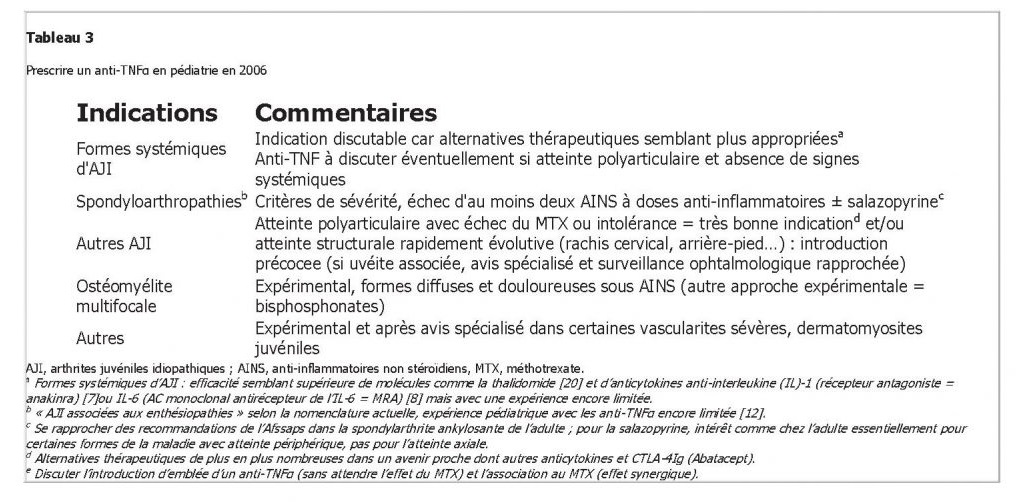
Le Tableau 3 résume les indications qui nous paraissent solides ou envisageable de traitement par anti-TNF chez l’enfant début 2006. Le bilan préthérapeutique et le suivi du traitement peuvent s’inspirer des recommandations récemment publiées dans ce journal par un ensemble d’expert rhumatologues et internistes d’adultes sous l’égide du Club rhumatisme et inflammations [19,21,22]. L’association au MTX, synergique, peut être considérée dans certaines situations de contrôle thérapeutique difficile sous anti-TNF seul. Les associations anti-TNFα–autre agent biologique apparaissent encore trop expérimentales pour être proposées chez l’enfant.
Références
- [1] Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al., International League of Associations for Rheumatology. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol 2004;31:390–2.
- [2] Hofer MF, Mouy R, Prieur AM. Juvenile idiopathic arthritides evaluated prospectively in a single center according to the Durban criteria. J Rheumatol 2001;28:1083–90.
- [3] Lovell DJ, Giannini EH, Reiff A, Cawkwell GD, Silverman ED, Nocton JJ, et al. Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group. N Engl J Med 2000;342:763–9.
- [4] Quartier P, Taupin P, Bourdeaut F, Lemelle I, Pillet P, Bost M, et al. Efficacy of etanercept for the treatment of juvenile idiopathic arthritis according to the onset type. Arthritis Rheum 2003;48:1093–101.
- [5] Horneff G, Schmeling H, Biedermann T, Foeldvari I, Ganser G, Girschick HJ, et al., Paediatric Rheumatology Collaborative Group. The German etanercept registry for treatment of juvenile idiopathic arthritis. Ann Rheum Dis 2004;63:1638–44.
- [6] Lovell DJ, Giannini EH, Reiff A, Jones OY, Schneider R, Olson JC, et al. Long-term efficacy and safety of etanercept in children with polyarticular-course juvenile rheumatoid arthritis: interim results from an ongoing multicenter, open-label, extended-treatment trial. Arthritis Rheum 2003;48:218–26.
- [7] Pascual V, Allantaz F, Arce E, Punaro M, Banchereau J. Role of interleukin-1 (IL-1) in the pathogenesis of systemic onset juvenile idiopathic arthritis and clinical response to IL-1 blockade. J Exp Med 2005; 201:1479–86.
- [8] Yokota S, Miyamae T, Imagawa T, Iwata N, Katakura S, Mori M, et al. Therapeutic efficacy of humanized recombinant anti-interleukin-6 receptor antibody in children with systemic-onset juvenile idiopathic arthritis. Arthritis Rheum 2005;52:818–25.
- [9] Sicotte NL, Voskuhl RR. Onset of multiple sclerosis associated with anti- TNF therapy. Neurology 2001;57:1885–8.
- [10] Tubach F, Salmon-Ceron D, Ravaud P, Mariette X, for the RATIO Study Group. The RATIO observatory: French registry of opportunistic infections, severe bacterial infections, and lymphomas complicating anti- TNFα therapy. Joint Bone Spine 2005;72:456–60.
- [11] Hawrot AC, Metry DW, Theos AJ, Levy ML. Etanercept for psoriasis in the pediatric population: experience in nine patients. Pediatr Dermatol 2006;23:67–71.
- [12] Tse SM, Burgos-Vargas R, Laxer RM. Antitumor necrosis factor alpha blockade in the treatment of juvenile spondylarthropathy. Arthritis Rheum 2005;52:2103–8.
- [13] Rajaraman RT, Kimura Y, Li S, Haines K, Chu DS. Retrospective case review of pediatric patients with uveitis treated with infliximab. Ophthalmology 2006;113:308–14.
- [14] Richards JC, Tay-Kearney ML, Murray K, Manners P. Infliximab for juvenile idiopathic arthritis-associated uveitis. Clin Experiment Ophthalmol 2005;33:461–8.
- [15] Reiff A. Long-term outcome of etanercept therapy in children with treatment-refractory uveitis. Arthritis Rheum 2003;48:2079–80.
- [16] Norman R, Greenberg RG, Jackson JM. Case reports of etanercept in inflammatory dermatoses. J Am Acad Dermatol 2006;54(3 Suppl 2): S139–42.
- [17] Deutschmann A, Mache CJ, Bodo K, Zebedin D, Ring E. Successful treatment of chronic recurrent multifocal osteomyelitis with tumor necrosis factor-alpha blockage. Pediatrics 2005;116:1231–3.
- [18] Tynjala P, Lahdenne P, Vahasalo P, Kautiainen H, Honkanen V. Impact of anti-TNF therapy on growth in severe juvenile idiopathic arthritis. Ann Rheum Dis 2006 (Jan 31; [Epub ahead of print]).
- [19] Pham T, Claudepierre P, Deprez X, Fautrel B, Goupille P, Hilliquin P, et al., Club Rhumatismes et Inflammation, French Society of Rheumatology. Anti-TNF α therapy and safety monitoring. Clinical tool guide elaborated
- by the Club Rhumatismes et Inflammations (CRI), section of the French Society of Rheumatology (Societe Francaise de Rhumatologie, SFR). Joint Bone Spine 2005;72(Suppl 1):1–58.
- [20] Lehman TJ, Schechter SJ, Sundel RP, Oliveira SK, Huttenlocher A, Onel KB. Thalidomide for severe systemic onset juvenile rheumatoid arthritis: A multicenter study. J Pediatr 2004;145:856–7.
- [21] Pham T, Guillemin F, Claudepierre P, Luc M, Miceli-Richard C, Fautrel F, et al. TNFα antagonist therapy in ankylosing spondylitis and psoriatic arthritis: recommendations of the French Society for Rheumatology.
Joint Bone Spine 2006 (in Press). - [22] Fautrel B, Constantin A, Morel J, Vittecoq O, Cantagrel A, Combe B, et al. Recommendations of the French Society for Rheumatology. TNFα antagonist therapy in rheumatoid arthritis. Joint Bone Spine 2006;73: 433–41.

